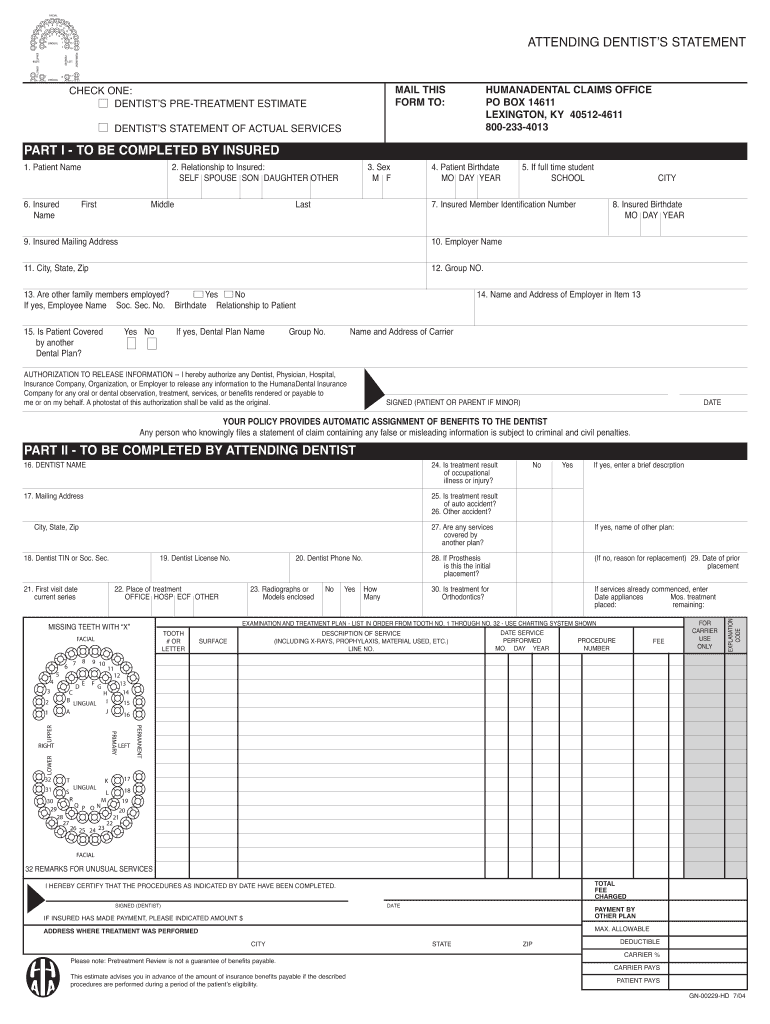
Printable Ada Dental Claim Form 2012
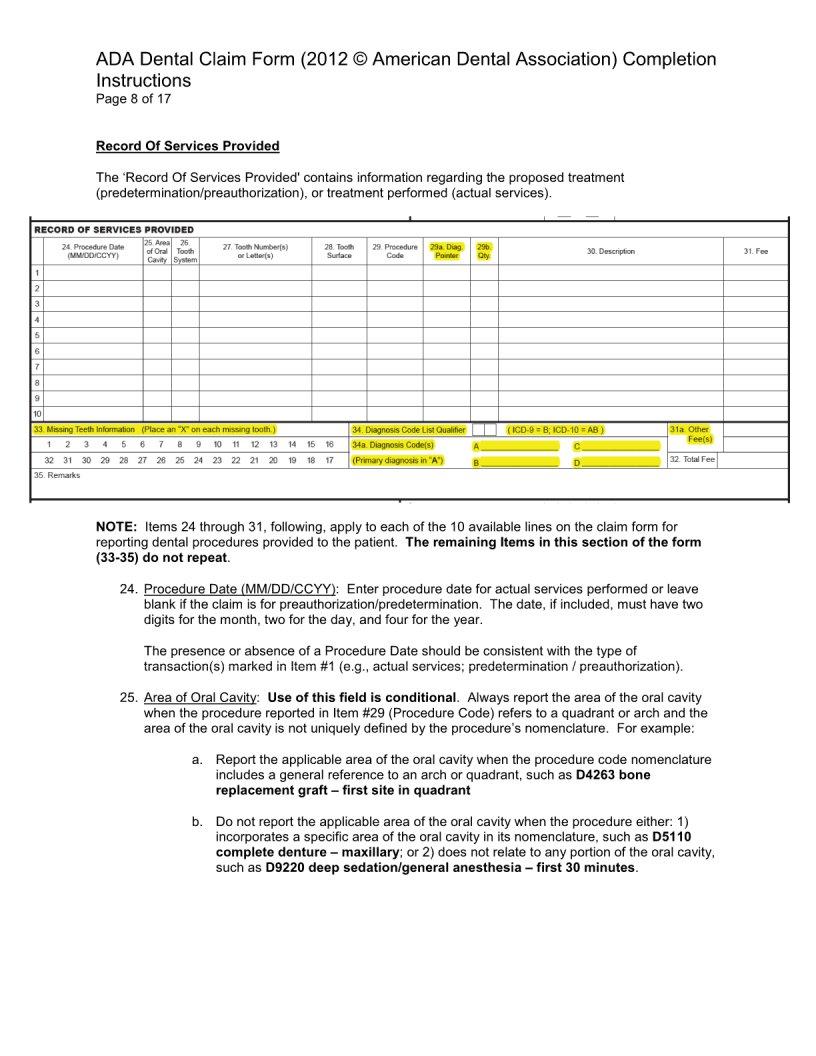
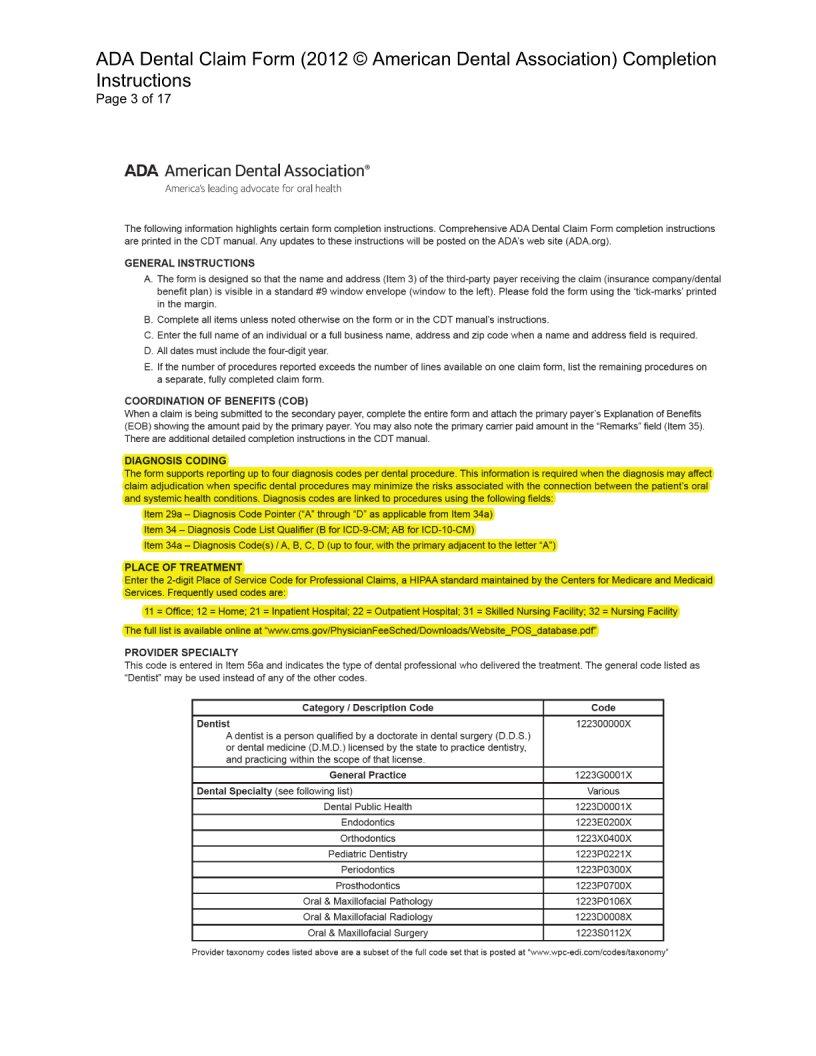
Printable Ada Dental Claim Form 2012 - Request a cdt code addition, revision, or deletion. Ada american dental association header information i typo of transaction (mark a applicable boxes) dental claim form policyholdewsubscriber information company in name (last, city. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. (leave blank if dentist or dental entity is not submitting claim on behalf of the patient or insured/subscriber) 48. Check ‘yes’ to indicate other. Get the new cdt 2025 kit for your practice! Any updates to these instructions will be posted on the ada’s web site (ada.org). Dental and orthodontic services must be billed on the ada 2012 dental claim form. If the patient has a primary insurance, then an attached eob is required. Ada news articles related to cdt codes. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Ada american dental association header information i typo of transaction (mark a applicable boxes) dental claim form policyholdewsubscriber information company in name (last, city. The form is designed so that the primary payer's name and address (item 3) is visible in a standard #10 window envelope. Blue cross and blue shield of illinois Name, address, city, state, zip code. (leave blank if dentist or dental entity is not submitting claim on behalf of the patient or insured/subscriber) 48. Cdt publications with misprints or omissions. Up to $40 cash back the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Any updates to these instructions will be posted on the ada’s web site (ada.org). Zip statement ot actual servxes request 2. Dental and orthodontic services must be billed on the ada 2012 dental claim form. Ada american dental association header information i typo of transaction (mark a applicable boxes) dental claim form policyholdewsubscriber information company in name (last, city. Please complete every item on claim form. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. The ada. Check ‘yes’ to indicate other. Any updates to these instructions will be posted on the ada’s web site (ada.org). Dental and orthodontic services must be billed on the ada 2012 dental claim form. This completed form, together with the itemized bills, should be submitted to: Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Please complete every item on claim form. Ada dental claim form header information 1. Cdt publications with misprints or omissions. View and download teamcare forms and documents in the following categories: Please complete every item on claim form. If the patient has a primary insurance, then an attached eob is required. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Ada dental claim form header information 1. Zip statement ot actual servxes request 2. Any updates to these instructions will be posted on the ada’s web. Name, address, city, state, zip code. Blue cross and blue shield of illinois Up to $40 cash back the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Type of transaction (mark all applicable boxes). The ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Up to $40 cash back the ada dental claim form provides a common format for reporting dental services to a. Blue cross and blue shield of illinois Cdt publications with misprints or omissions. Instructions for completing the ada dental claim form. Ada news articles related to cdt codes. Zip statement ot actual servxes request 2. Cdt publications with misprints or omissions. Blue cross and blue shield of illinois Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Blue cross and blue shield of illinois Check ‘yes’ to indicate other. Dental and orthodontic services must be billed on the ada 2012 dental claim form. Please complete every item on claim form. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Any updates to these instructions will be posted on the ada’s web site (ada.org). This completed form, together with the itemized bills, should be submitted to: Ada american dental association header information i typo of transaction (mark a applicable boxes) dental claim form policyholdewsubscriber information company in name (last, city. Instructions for completing the ada dental claim form. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. View and download teamcare forms and documents in the following categories: Ada dental claim form. Any updates to these instructions will be posted on the ada’s web site (ada.org). Any updates to these instructions will be posted on the ada’s web site (ada.org). This completed form, together with the itemized bills, should be submitted to: Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. Up to $40 cash back the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Blue cross and blue shield of illinois The ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into the now current version of the hipaa standard (837d v5010) electronic dental claim. Name, address, city, state, zip code. If the patient has a primary insurance, then an attached eob is required. Request a cdt code addition, revision, or deletion. The ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Please complete every item on claim form. Zip statement ot actual servxes request 2. The form is designed so that the primary payer's name and address (item 3) is visible in a standard #10 window envelope.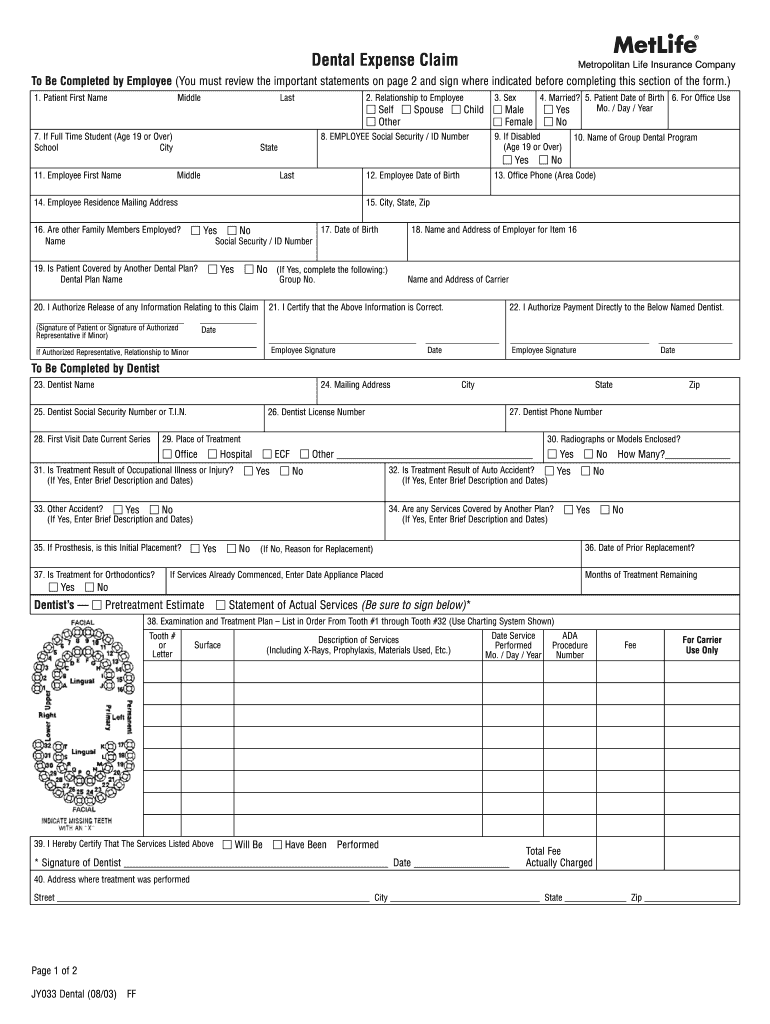
Ada Dental Claim Form Blank Fill Online Printable Fillable Blank
Ada Form Dental ≡ Fill Out Printable PDF Forms Online

Fillable Online medicaid ms ADA Dental Claim Form (2012American Dental
Blank Printable Ada Dental Claim Form A) Services Delivered By A
Ada Form Dental ≡ Fill Out Printable PDF Forms Online

ADA Dental Insurance Forms
Free Printable Ada Dental Claim Form

Ada Dental Claim Form Blank Fill Online Printable Fillable Blank
Printable Ada Dental Claim Form 2012

Printable Ada Dental Claim Form 2024
(Leave Blank If Dentist Or Dental Entity Is Not Submitting Claim On Behalf Of The Patient Or Insured/Subscriber) 48.
Ada News Articles Related To Cdt Codes.
Type Of Transaction (Mark All Applicable Boxes).
Ada American Dental Association Header Information I Typo Of Transaction (Mark A Applicable Boxes) Dental Claim Form Policyholdewsubscriber Information Company In Name (Last, City.
Related Post: